








Since our last update, US coronavirus cases have surged higher than we expected for several reasons.
In an interview in June, Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, said transmission for Covid-19 won’t follow the wave pattern we have seen with influenza pandemics. He expects ongoing transmission in the US could look more like a slow burn, likening the pandemic to a forest fire and uninfected individuals to remaining wood to burn, with hills and valleys in the outbreak in different regions.
Updated Forecast: Death Rates, Infection Rates, and Tests
Our updated US coronavirus forecast assumes 274,000 deaths and nearly 20% infected by the end of 2020. Daily US diagnoses bottomed out in May around 20,000 but steadily climbed in June and July and remained high in August at around 50,000 per day.
Hospitalisations and deaths tend to lag diagnoses; on average, it takes five days for a person to develop symptoms, but it can take weeks for a patient to die from Covid-19. Cases seem to be skewing younger, leading to a lower death rate, but daily US deaths are now typically back above 1,000 a day after dipping below this for June and the first half of July.
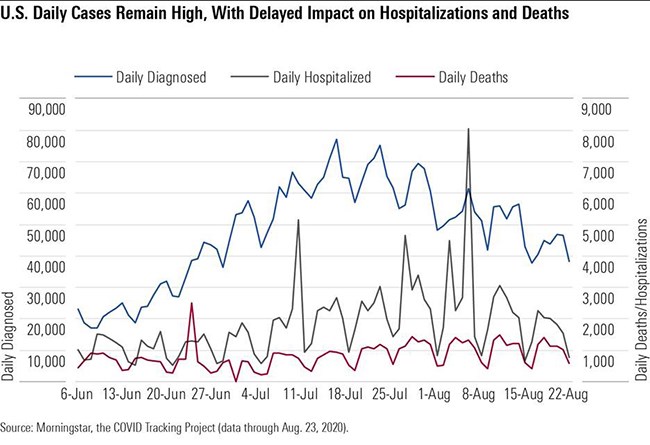
The death rate is also falling, probably because cases today are averaging at a lower age (likely influenced by the reopening of restaurants and bars and better safeguards around long-term care facilities). It’s also possible that hospitals are getting better at treating severely ill patients, with better access to drugs like remdesivir and dexamethasone and better standards of care.
But while a surge may start in a healthier, younger population, it’s hard to keep infections isolated from older populations in the long-run if infection levels in society remain higher. Moreover, epidemiologists estimate that the US is still only diagnosing roughly 10% of cases, meaning that most infected individuals are in a position to unknowingly infect their close contacts.
Diagnostic Testing Hits its Limit
The daily volume of Covid-19 diagnostic tests has grown significantly over the past two months, but the lack of centralised testing management in the US has led to local supply shortages and difficulty matching supplies with available platforms. Demand has also intensified, outstripping the supply of kits.
We expect incremental improvements in supply with better co-ordination of labs and pooled PCR testing (testing multiple samples together) but also potentially larger increases in supply this fall with the embrace of less sensitive but cheaper and much faster tests, including antigen tests and new CRISPR-based tests. Labcorp (LH) has improved to 180,000 daily tests and two- to three-day turnaround times, and Quest (DGX) plans to expand to 185,000 this month, also allowing two- to three-day turnarounds.
The Food and Drug Administration authorised Quest to pool samples from up to four patients and authorised LabCorp’s test to be used in asymptomatic individuals or pooled tests for up to five samples in July. Hologic (HOLX) filed for an emergency use authorisation (EUA) for its tests in August. These authorisations could be particularly helpful as we screen larger populations.
Antigen tests and new technologies could help achieve faster, point-of-care results and improve access to testing, but it could be several months before this becomes widespread, and current antigen tests involve some sacrifice in test accuracy. In late July, the National Institutes of Health announced a $250 million investment in seven diagnostics firms as the culmination of the Rapid Acceleration of Diagnostics (RADx) initiative, which could boost diagnostics access by millions per week beginning in September.
The RADx goal will require increased use of antigen-based tests and novel test approvals. Antigen tests detect proteins made by the virus. The first, by Quidel (QDEL), was approved in May and rolled out in urgent care centres. A second approved antigen test from Becton Dickinson (BDX) can produce results in 15 minutes.
We’re encouraged by the news of Abbott’s (ABT) EUA for a 15-minute lateral flow antigen test, which will be priced at $5. Because this requires no equipment (although it does require a healthcare professional to administer the nasal swab), it will bypass the bottlenecks at labs. A complementary app will allow those who test negative to show a health pass for entry into facilities. Scale is critical to the test’s relevance, and we think this could have a significant impact on testing by October.
Newer technologies that can amplify genes using CRISPR gene editing technology or use chemicals to detect small amounts of virus could also allow for fast and perhaps more sensitive point-of-care testing than Abbott’s RT-PCR point-of-care test and Quidel’s and BD’s antigen tests. The first CRISPR-based diagnostic, from Sherlock Biosciences, has been approved by the FDA, and Glaxo (GSK) and Mammoth Biosciences are working on another, even faster (20-minute) CRISPR-based test. Also, a saliva-based testing method from Yale was granted an EUA in mid-August; given that the technology is open for other labs to use and does not require special collection tubes, this could be another avenue to opening up testing capacity.
Antivirals and Other Coronavirus Treatments
While we’ve previously cited the 10% positive rate benchmark as the one given by the World Health Organisation to control a pandemic, the WHO advised on May 12 that a 5% positive rate was necessary for countries to reopen safely, and the Harvard Global Health Institute’s recommendations translate to a 10% positive rate for stabilisation and a 3% positive rate for suppression.
Positive rates lower than 1.5% have been achieved in several European countries. However, data from the US over the week of August 8-15 shows that few states are achieving the 3% positive rate needed for suppression, with most teetering near the boundary between stability and growth
Meanwhile, progress with coronavirus treatments has been mixed. By the end of the year, we expect data on new antivirals and whether combinations of Gilead's (GILD) remdesivir combinations with oral antivirals like Pfizer’s (PFE) protease inhibitor or Merck/Ridgeback’s (MRK) EIDD-2801 improve on remdesivir alone.
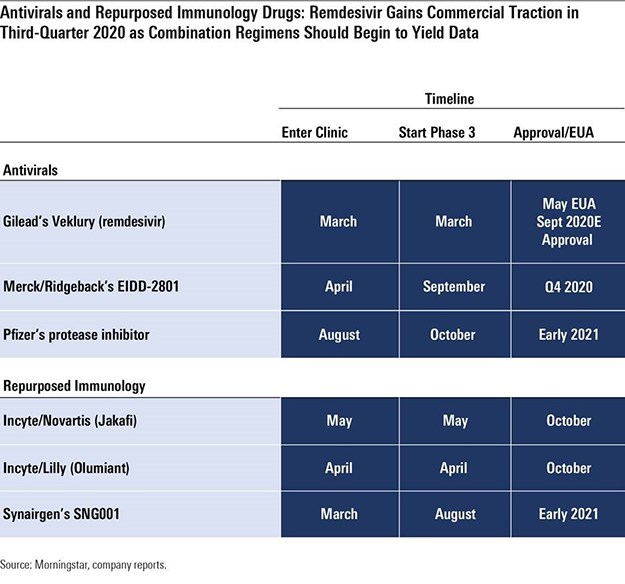
- Remdesivir We think remdesivir has a place in the near- to mid-term as a treatment for patients hospitalised with Covid-19 but not yet on mechanical ventilation, although we expect vaccines and other coronavirus treatments to reduce demand significantly beyond 2021, and we only model sales through 2023. We assume peak sales of nearly $3 billion in 2020, using a $2,340 price and 1.2 million treated commercial patients as our key assumptions. Gilead also started a phase 1 trial of inhaled remdesivir in healthy volunteers in July, with the aim of testing this method of administration in Covid-19 patients in August. An inhaled version could allow Gilead to treat non-hospitalised patients, potentially preventing hospitalisation in some patients (the current infused version would be difficult to extend into healthier patients). Overall, we estimate that roughly 1.2 million patients could receive the commercial drug in the second half of 2020 at the five-day dosing schedule.
- EIDD-2801 is an oral nucleoside analog that has shown pre-clinical efficacy as a coronavirus treatment and preventive antiviral in SARS and MERS; the drug improved pulmonary function, decreased weight loss, and reduced the amount of virus in the lungs. In its phase 1 trial, which started in the UK in April, the drug had solid tolerability data, leading Ridgeback to start two phase 2 studies in June, testing whether patients become free of virus. Ridgeback expects to have 1 million courses available by autumn, and a phase 3 trial is planned to start this month, which we think could allow the drug to compete with remdesivir in 2021 and expand its reach into patients who are sick at home, where intravenous remdesivir is not practical.
- SNG001 the inhaled interferon from Synairgen (SYGGF), offered promising data in July that pointed to reduced potential for developing severe disease and greater likelihood of recovery for patients taking the drug versus those on placebo. The SNG001 study had only roughly 100 hospitalised patients, Synairgen did not publish information on the primary endpoint (28-day improvement), and it is unclear if the results are statistically significant; however, injectable beta-interferon is now entering an NIH-sponsored study in combination with remdesivir.
- JAK inhibitors Olumiant and Jakafi are expected to provide data in the coming months, although repurposed immunology drugs so far have a poor record, with IL-6 antibodies Actemra and Kevzara failing to improve outcomes.
Passive Immunisation as a Coronavirus Treatment
Passive immunisation involves administering antibodies to prevent disease. Unlike vaccination, it does not require the patient to mount an immune response in order for the antibodies to be effective. These antibodies can be from a recovered patient (convalescent sera) or from a lab (engineered monoclonal antibodies designed for similarity to the most potent neutralising antibodies from natural infection). We expect monoclonal antibody therapies have more promise than convalescent sera, as they provide a more uniform product, are likely more effective, and can be made at a much larger scale.
We expect demand for these antibodies to be highest before an effective Covid-19 vaccine is available but also significant on a smaller scale afterward (to treat unvaccinated individuals or as prophylaxis in those for whom a vaccine is ineffective).
Antibodies could be particularly useful as coronavirus treatments and preventive measures for older adults at high risk of exposure, as older adult immune systems may not respond as well to vaccination.
Elsewhere, Operation Warp Speed has signed a contract with Regeneron (REGN) for its engineered monoclonal antibodies (based partly on the most effective antibodies produced during natural infection). A cocktail of two such antibodies, which entered testing in June, could be less likely than other antibody programs to lead to resistant viral mutations. While antibodies are among the most promising therapies for Covid-19, hurdles remain due to cost, manufacturing capacity, and the expected duration of protection.
However, Regeneron’s recent deal with Roche (RO) expands manufacturing capacity, and several other antibody programs - from companies including AstraZeneca (AZN) and Lilly (LLY) - have entered clinical trials.
Overall, we see Regeneron’s antibody cocktail as highly likely to receive an FDA EUA this year, and assume a 60% probability of approval despite a current lack of clinical data.
Regeneron started two clinical studies for antibody cocktail REGN-COV2 in June, and late-stage development as a coronavirus treatment began in July; the company expects initial data in September. It is also conducting a prevention study with the National Institute of Allergy and Infectious Diseases that began in July. We assume emergency use could beginin autumn.
Regeneron is quickly ramping up manufacturing capacity for the cocktail and will potentially supply millions of doses per month from its New York facility by 2021. Given the significant increase in manufacturing capacity, we now assume $6 billion in probability-adjusted peak sales in 2021 ($10 billion in sales, if approved), with roughly half the economics going to Regeneron and the other half to Roche (50%-60% of worldwide gross profits are expected to go to Regeneron).
Several other antibody programs are entering diagnostic testing, but Regeneron’s program is the most advanced and is distinguished from most with its cocktail strategy. We assume sales decline beyond 2021 and disappear by 2023, as vaccination rates in society should lead to herd immunity, reducing the need for ongoing coronavirus treatment or preventive therapy with antibodies.
This article first appeared on Morningstar US





















